
By Michael Traum, MD, PGY-1 | Edited by Leila PoSaw, MD, Ultrasound Director
Download a printer-friendly version of the FASH Exam here
As a first-year resident, the story of the Focused Assessment with Sonography for HIV/TB, or the FASH exam, is nothing short of inspiring, and I would like to share this with you.
While working at a rural district hospital in South Africa, Dr. Tom Heller came up with a simple yet powerful idea: the transformation of the traditional FAST exam into the novel FASH exam. Dr. Heller was inspired by his very sick HIV/TB patients who suffered due to the lack of availability of sophisticated imaging modalities. For these sick patients, early diagnosis is crucial for appropriate treatment. Dr. Heller took the simple, readily available, ultrasound machine and developed a protocol that has been adopted by clinicians around the world.
The FASH exam was developed in 2010 to rapidly diagnose extrapulmonary and disseminated TB in patients infected with HIV. It is a focused, integrated, goal directed, bedside examination. The protocol asks simple binary questions (yes/no). It is clinically relevant to the immediate treatment of the patient and easily performed by healthcare staff with minimal training.
The FASH exam is recommended in HIV prevalent settings (rates >5%), in patients with known or suspected HIV and in whom you highly suspect extrapulmonary, smear negative TB. These patients usually appear sick and may present with chest pain, dyspnea, hypotension, abdominal pain or fever.
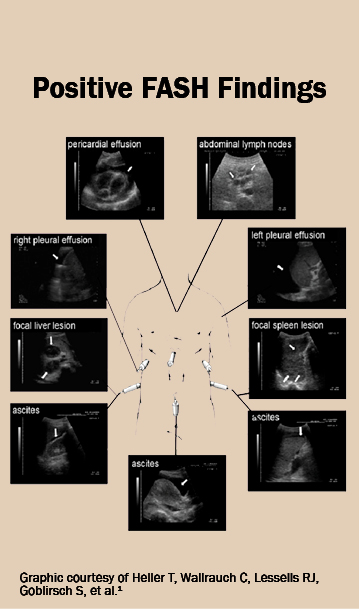
The main objective of the FASH exam is to detect pleural and pericardial effusions, enlarged abdominal lymph nodes, and focal spleen and liver lesions – all suggestive of disseminated extrapulmonary TB.
The following six questions (yes/no) are asked:
- Is there a pericardial effusion?
- Is there a pleural effusion?
- Is there free fluid in the abdomen?
- Are there periportal/para-aortic lymph nodes?
- Are there focal liver lesions?
- Are there focal spleen lesions?
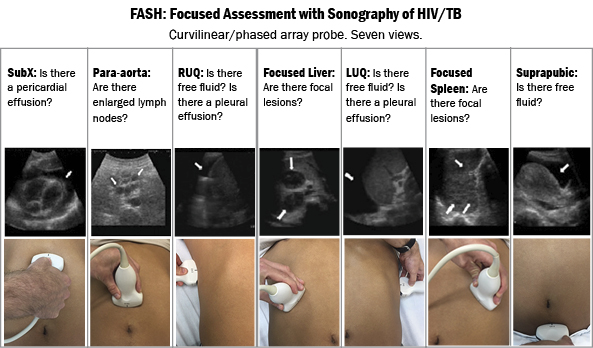
Seven views are obtained with the curvilinear or phased array probe.
- The Subxiphoid view evaluates for the presence of pericardial effusion.
- The Para-aortic view assesses for the presence of enlarged abdominal lymph nodes. These appear as hypoechoic, round structures which may appear to grow or shrink when fanning through the image. Enlarged lymph nodes >1.5 cm are highly suggestive of disseminated abdominal TB.
- The RUQ view assesses for the presence of pleural effusion and for free fluid. Pleural effusions are typically anechoic or hypoechoic; however, effusions from TB may be fibrinous with a heterogeneous sonographic appearance. Similarly, patients with TB may have hypoechoic ascites or may exhibit fibrinous strands.
- The Focused Liver view evaluates for focal, hypoechoic liver lesions.
- The LUQ view assesses for pleural effusions in the left lung. Unilateral pleural effusions are more common in TB. This view also assesses for free fluid in the spleno-renal space.
- The Focused Spleen view evaluates the spleen to look for the focal, hypoechoic lesions which are often due to disseminated TB. These abscesses have a characteristic appearance and should prompt confirmatory studies.
- The final view of the FASH exam is the Suprapubic view to evaluate for ascites. While not specific, this view is crucial for completeness.
The FASH exam was not designed to replace detailed comprehensive imaging. It is meant as a technique to quickly assess critically ill patients, especially in resource-poor environments. Ultrasound is user-dependent, most valuable when the pretest probability is high, and is a rule-in test rather than a rule-out. Keep in mind that effusions can be due to multiple causes, including other opportunistic infections in patients with HIV. Also, liver and spleen findings can be caused by amebic or other infections especially in endemic, tropical regions.
I practice at Jackson Memorial Hospital, which is a county hospital in Miami, Florida. We care for a large number of underserved and foreign-born patients. According to the CDC, the rate of TB in foreign-born persons is nearly nine times higher than that of those born in the U.S., and the Miami metropolitan area has the highest rates of new HIV diagnoses in the country. While we do not have higher than 5% HIV prevalence rates, I will be on the alert for positive FASH findings in my immunosuppressed, sick patients. I have a sneaky suspicion that having this protocol in my toolbox will prove useful someday!